
Corrupting technology: An integrity check on the organ transplant industry
Abstract
This paper discusses aspects of organ donation and transplantation (ODT) as an example of technology delivering significant health and longevity benefits to patients, but fraught with ethical challenges and open to incidental or systematic corruption. The paper outlines the main features of current ethical debate on organ procurement and allocation, including allegations of illicit procurement and trade in human organs. It concludes by encouraging Baptists to retrieve and articulate the notion of the common good in order to focus attention on ‘public’ rather than ‘personal’ ethical issues and to foster a vision for biblically-based and theologically-driven social transformation.
1. What is organ donation and transplantation?
Organ transplantation is the replacement of worn-out, diseased or injured organs and tissues with healthy substitutes. It has become standard medical practice over the last forty years. ODT has the capacity to extend life, alleviate suffering, cure disease, restore normal body functioning, and reduce health costs (the latter because transplant, while relatively expensive, is often cheaper than maintaining the life and health of a chronically or terminally ill patient in need of new organs). Additionally, organs donated for research help improve medical knowledge and train practitioners.
More than 20 human organs, both regenerative and non-regenerative, are now transplantable. The most common organ and tissue transplants are the heart, lungs, kidneys, liver, pancreas, small intestine, cornea, nerve, skin, tendons, bone marrow and blood vessels. While a patient’s own regenerative organs may be used, usually transplantation requires organ donation from another human subject. Where this occurs, the recipient’s immune system normally identifies the donor tissue as foreign and seeks to destroy it by producing antibodies. The degree of genetic disparity between donor and recipient determines the degree and speed of this rejection. Close genetic matching, and the use of recently discovered drugs such as prednisone, azathioprine and cyclosporine, suppress the immune system’s response and increase the likelihood of a positive outcome. It can be argued that deaths resulting from waiting to receive an organ are preventable deaths. Moreover, it has been claimed[1] that one donor can help up to 32 people enjoy a better quality of life.
There are, however, many complex and contested ethical issues relating to ODT. Significant ethical issues include:
- What should determine the legal definition of death, given that organs removed for transplant must possess ‘life’ (brain death, cessation of heart function, or some other indicator)?
- Should healthy organs be removed from healthy live donors?
- Is it possible to eliminate manipulation and coercion of potential living donors who are related to the recipient?
- How should access to transplantation be determined?
- Who owns a body?
- What responsibility should the state assume for disposing of a body after death?
- How should medical professionals address the presumed rights and responsibilities of potential donors and their families?
- To what extent do donors and recipients have a right to privacy/anonymity?
- Is “presumed consent,” whereby agreement to donate organs at death is presumed unless the deceased previously requested otherwise, ethical or merely expedient?
- Should it be permissible to supply human organs and tissue in return for payment?
- Will persons who sign donor agreements receive the same medical treatment they would have received if they had identified as non-donors?
2. Medical and theological principles relating to ODT
As with any bioethical issue, a range of general principles drawn from medical and theological ethics may be applied to the challenges posed by ODT.
Medical principles
Four general principles summarise the main thrust of secular medical ethics and are discussed, with varying emphasis, in relation to ODT:
- Autonomy: respect for the individual, expressed in decision-making such as informed consent/refusal, and applying treatment in the best interests of the patient;
- Non-maleficence: an obligation not to inflict harm on others (“do no harm”);
- Beneficence: an obligation to contribute to the welfare of others (“do dood”);
- Justice: fair, equitable and appropriate treatment in the light of what is due or owed to persons.[2]
Theological principles
Three general theological principles, somewhat parallel to the four principles outlined above but distilled from Old and New Testament teachings, may also inform ethical discussions on ODT:
- Respect for persons: unconditional regard for the rights and responsibilities of others who are created in the image of God (cf the so-called ‘Golden Rule’: “In everything do to others as you would have them do to you; for this is the law and the prophets,” Matthew 7:12);
- Neighbour-love: affection and compassion toward others regardless of difference, perhaps best illustrated in the parable of the Good Samaritan (Luke 10:25-37; cf Philippians 2:4);
- Justice: a commitment to fair and equitable standards and processes that please God and contribute to shalom (e.g. Amos 5:21-24; Micah 6:8; Matthew 23:23).
3. Organ procurement and allocation
According to nineteenth century German politician Otto von Bismark, there are two things it is best not to know: how sausages are made, and how laws are made. If you want to enjoy the outcomes of the political process, don’t look too closely at the details. The same could be said of the organ transplant industry in the 21st century. For many people, however, transplant organs and tissues are valuable and life-saving commodities. Ethical issues relating to procurement and allocation include donor consent, sources of organs and tissue, methods of allocation, and the potential for commercial exploitation of vulnerable persons. There are also pastoral care and counselling issues but these are beyond the scope of this paper.
Consent to donate organs
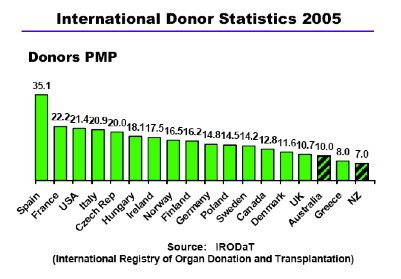
Demand for transplant organs far outweighs supply. In Australia, only one per cent of deaths occur in circumstances amenable to transplantation (i.e. the donor is healthy, young, in a hospital equipped for organ donation, and consent has been given). The peak national body regulating ODT in Australia claims that “difficulties associated with obtaining consent could be preventing donation in as many as one third of cases where deceased patients were identified as potential organ donors.”[3] According to polls, approximately 90 per cent of Australians favour organ donation,[4] but the donor rate is almost the lowest in the developed world (see Table 1).[5] Since 2000, the rate, expressed as the number of donors per million population, has ranged between 9 and 11 (in Spain the rate was 33.7 in 2002 and 35.1 in 2005).
TABLE 1[6]
There are three main approaches to consent:
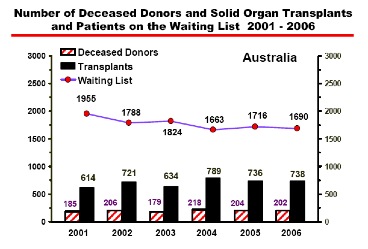
- Expressed (or informed) consent (“opt in”): organs may be removed from a deceased person for transplantation if the person has expressed a wish to donate their organs, and may not be removed if the person has expressed an objection to donating their organs. Where no preference is made, the family of the deceased is consulted about whether they believed the deceased would have wanted their organs donated for transplantation. In practice, however, even in cases where the deceased has registered a wish to donate their organs for transplantation, hospital staff will still consult the family and the deceased’s wishes can be overridden.[7] In Australia in 2006, there were 202 organ donors; authority for organ donation was sought in 65 per cent of cases by the Intensive Care Clinician, in eight per cent of cases by the Donor Coordinator, and volunteered by the family in 22 per cent of cases.[8] In some Australian states, intent to donate organs is registered on their driver’s licence, a practice which has led to the rise of urban myths of ambulance officers at car accidents checking the licences of seriously injured persons before deciding to resuscitate or treat. Table 2 shows the significant gap between the number of deceased donors and the number of persons on transplant waiting lists in Australia.
- Presumed consent (“opt out”): organs may be removed from a deceased person for transplantation if the person has not expressed an objection to donating their organs. There are two forms: in the “hard” version (practised in Austria), hospital staff are not required to consult the family of the deceased; in the “soft” version (practised in Spain and Belgium), the family is consulted about whether the deceased objected to donating their organs.
- Required request: in the United States, a potential donor’s next of kin must be asked to give consent before organs can be removed from a deceased person for transplantation.
TABLE 2[9]
In Australia, to be effective “consent must be freely made, given with respect to the precise procedure carried out, given by a person with legal capacity to give consent, given in writing, in words, or implied from conduct, or authorised by a court order. In addition, consent must not be obtained by fraud or duress, which makes difficult the process of obtaining consent from people in the custody of the state, such as prisoners.”[10] National organ donation registries may also be established to encourage decision-making about organ donation. In Australia, the Health Insurance Commission has administered a registry since 2000 (now administered by Medicare), but there has been no identifiable impact on donation statistics.[11]
To increase supply of donor organs and reduce transplant waiting lists, governments may legislate to make it easier for hospitals to acquire donor organs and tissue. This also has the effect of reducing the cost of public health, as the cumulative costs associated with maintaining a patient on a transplant waiting list normally exceed the costs associated with transplantation. Governments must take care not to appear coercive, and not to be motivated by cost-saving, in seeking to change laws relating to ODT. Where there is a fear of coercion, or abrogation of rights, donation plummets. In addition, various cultural and religious factors discourage organ donation.
Sources and methods of procurement
The serious shortfall in supply of organs suitable for transplant increases the impetus for accepting organs from living donors (e.g. one kidney), increases pressure to allow commercial trade in organs, and encourages unethical procurement practices. Various ethical issues arise in public policy debates on increasing the supply of organs and tissue for transplantation:[12]
- Use of cadaver organs as indicated in the previous section;
- Use of living donors of renewable tissues (such as skin and bone marrow) and nonvital or paired organs (such as kidneys): questions of manipulation and coercion by family members;
- Use of tissue from aborted foetuses and anencephalic donors (babies born with a brain stem but lacking a higher brain, which usually die soon after birth);
- Use of tissue, and potentially of laboratory-cultivated organs, from stem cell lines;
- Use of organs and tissue from cloned humans;
- Use of organs and tissue from other species (xenotransplantation);
- Markets in organs and tissues: either to increase supply, or to respect the freedom of individuals to do as they wish with their lives as long as they do no harm to others;
- Questions of macroallocation (how much of a good should be made available?), and microallocation (who should receive that good when its supply is limited?).
Here I will focus briefly on the last two issues, involving economics and human rights – issues which tend to attract less acrimonious debate and therefore less interest within the Christian community than is generated in relation to the use of foetal and stem cell tissue, cloning and xenotransplantation.
It is fair to say that there is an acute and growing international shortage of organs and tissue for transplantation. Such an environment increases the potential for morally dubious and even criminal behaviour on the part of government authorities, commercial interests, and individual medical practitioners and consumers. This is well documented; indeed in addition to media stories celebrating life-saving transplantations, a significant proportion of stories on ODT feature sensational allegations of so-called “organ harvesting” and “transplant tourism.” For example:
- In the late 1980s it was alleged that transplant kidneys obtained from Chinese prisoners executed in Canton had sold for $11,000; and that, according to Chinese sources, such trade was ethical “as the criminals are making use of their last virtue.”[13]
- In 1988, German businessman Count Rainer Rene Adelmann zu Adlemannfelden announced the introduction of a legal “Organ Bureau” in 1989, offering to pay bankrupt business executives US$44,000 for a kidney and act as a middleman in transplant operations.[14]
- In 1989 four impoverished Turkish donors travelled to London and each had one kidney removed and transplanted into wealthy recipients at the private Humana Hospital. The donors were paid between AU$5000 and AU$7000, while those who brokered the deal allegedly received much higher sums. Subsequently the main broker in Turkey, Tunc Kunter, was convicted of “cheating people of their body organs” and sentenced to two years imprisonment; all British surgeons who performed the operations were convicted of serious professional misconduct; and the principal Harley Street specialist involved had his name removed from the British medical register. The defence in this case was that all the donors claimed to be related to the recipients, thus meeting British live organ donation criteria.[15]
- The same Harley Street specialist was also charged with professional misconduct over allegations of queue jumping, whereby wealthy foreigners paid large fees to gain priority treatment ahead of 3600 National Health Scheme patients awaiting transplants.[16]
- Allegations of baby trade in which Brazilian children were sent to Europe, ostensibly for adoption, and were later murdered and their hearts, kidneys and testicles sold “for between $40,000 and $100,000.[17]
- In the Philippines, where organ commerce is legal, prisoners may have their sentences shortened in return for kidney donation.[18]
- Unconfirmed reports suggest that US interests sold human kidneys to private British hospitals “because they were too old for use by American surgeons fearful of litigation.”[19]
- Allegations of organ theft by an unscrupulous doctor in India, where a patient admitted to hospital with abdominal pain had a kidney removed and was later “rewarded” with money from the Middle Eastern recipient.[20]
- In 1996 two Sudanese businessmen allegedly purchased organs from poor Egyptians and sold them to wealthy Arabs for commission.[21]
- It is alleged that government and health officials in China frequently offer to sell various organs and tissue for transplant in wealthy foreigners, sourced from executed criminals. For example, in one case there are extraordinary claims of “criminals executed by shooting in the body rather than the head so as not to damage the eye tissue [for cornea transplants] … [others] put to death by having essential organs removed, while some were not completely killed in order to preserve live tissue.” The brokers were later arrested in New York and faced penalties of up to five years imprisonment and fines of AU$595,000.[22]
- Activists have called for Western countries to “oppose the forced organ harvesting of prisoners in China”; and Professor Stephen Wigmore, chair of the ethics committee of the British Transplantation Society, called for “a full, frank international enquiry into China’s organ harvesting,” and urged transplantation agencies to agree on a public statement condemning the practice.[23]
- In Australia there are allegations of patients travelling overseas to receive transplant surgery; often these allegations refer to harvesting organs from Chinese prisoners of conscience, including former asylum seekers in Australian detention centres who had been deported.[24] A detailed report by human rights lawyers, commissioned by a Washington-based NGO and published in January 2007, concluded that:
the government of China and its agencies in numerous parts of the country, in particular hospitals but also detention centres and ‘people’s courts’, since 1999 have put to death a large but unknown number of Falun Gong prisoners of conscience. Their vital organs, including kidneys, livers, corneas and hearts, were seized involuntarily for sale at high prices, sometimes to foreigners, who normally face long waits for voluntary donations of such organs in their home countries.[25]
- Video footage of investigations documenting alleged organ trade in China is available on YouTube.[26]
Methods of allocation
Organs and tissues for transplantation may be allocated in four main ways:[27]
- Need: priority is given to those patients whose need is most urgent, or whose condition is most serious;
- Merit: priority is given to those judged to have the greatest social worth or potential to contribute to society;
- Outcome: resources are used where they are likely to deliver the greatest benefit (e.g. quality of life for a given cost);
- Random allocation: an alternative to all forms of prioritising where resources are distributed by a system such as a lottery or a first-come first-served rule.
Certainly issues of allocation are important for ethical reflection and deliberation. But as Neil Messer observes, “[i]n practice, policies may contain elements of different criteria, and it may sometimes be difficult to differentiate between the various criteria that may be operating in a particular case.”[28] In addition, the rationale for allocation decisions made by individual hospitals may be subjective and difficult to identify; they may even occasionally be made on an irrational basis.
Summary
It appears that a small number of business, medical and government persons negate the basic medical and theological principles relevant to ODT in at least three ways: first, by contravening humane laws in pursuit of monetary gain; second, by taking advantage of clients’ greed and/or fear; and third, by exploiting vulnerable people such as students, prisoners, the poor, and the naïve. Moreover, if news and investigative reports are accurate, the incidence of unethical practices relating to ODT is increasing, especially in China where the number of executions per year delivering viable and saleable organs to the state is allegedly in the tens of thousands.
4. ODT and the common good
One way of addressing the ethical challenges of ODT is to view them in the light of the principle of the common good, prominent in Catholic social teaching and amenable to the medical and theological principles outlined above, but rarely articulated in Baptist ethical thought and praxis. The notion of the common good appears to have originated in classical Greek thought. It was a transcultural idea and it is therefore not surprising to see it reflected to some degree in biblical teaching on justice.
In the Old Testament, the key terms are justice (mishpat) and righteousness (tsedaqah), often used together.[29] Both terms possess a social dimension,and convey a meaning close to the concerns of “social justice” as we might understand the term today.[30] The people of God are called to live in accordance with divine justice, and to model it in their relations with others; it is on this basis that their works will be judged.[31] Biblical righteousness/justice “is about the proper structure of relationships between God and people, and among human beings … [it] is not a virtue or quality which an individual can have in isolation.”[32]
In English usage, ‘righteousness’ is often associated with the notion of personal moral rectitude, while ‘justice’ generally signifies a right social order, evidenced by the proper distribution of goods, relations between persons, and retribution for evil. Righteousness typically pertains to matters of piety and religion; justice to legal and social issues.[33] In biblical usage, however, such a distinction is not apparent.[34] A related term is shalom, variously translated as “peace” or “wholeness,” conveying Yahweh’s intention for the whole human community and indeed the entire created order.[35]
This concern for justice and wholeness is reflected in the New Testament. Mary emphasises justice in her song in Luke 1:46-55. Jesus affirmed his mission as one of justice (Lk 4:14-21). He confronted those who denied justice to the poor, associated with those to whom justice had been denied, and encouraged people to pursue righteousness, justice and peace. The New Testament letters, particularly James, convey a preferential concern for the weaker members of the community, and address issues of conflict and injustice. Jesus himself “went about doing good,” apparently indiscriminately (Acts 10:38). Paul enjoined the Christians at Corinth to work together “for the common good” (1 Cor 12:7, NIV).
A similar idea appears in Luke 10:25-37 and Matthew 25:31-46 and elsewhere. The common good is not a synonym for social justice, but the desire for justice and wholeness expressed in human community implies a commitment by the people of God to the common good. Christian ethical concerns relating to ODT might be usefully framed in the light of the common good as an expression of a universal human ideal supported by the biblical teaching on justice and peace.
Speaking philosophically rather than theologically, one of the earliest extant references to the common good is in relation to Aristotle’s notion of the good life. His conception of morality found its centre in the “conviction that a good life is one devoted to the pursuit of good purposes or ends.”[36] He recognised the tension between what we might call individual rights and community responsibility, but took a communitarian view of the good:
Even if the good is the same for the individual and the city, the good of the city clearly is the greater and more perfect thing to attain and to safeguard. The attainment of the good for one person alone is, to be sure, a source of satisfaction; yet to secure it for a nation and for cities is nobler and more divine.[37]
Leading Christian theologians, most notably Thomas Aquinas, affirmed the primacy of the common good over the particular goods of individuals, and picked up on Aristotle’s allusion to a religious dimension. Thomas advanced two reasons for the superiority of the common good over its private counterpart. First, one may judge the goodness of a person only in relation to the extent that the common good is his/her goal (the argument of quantification).[38] Second, the right ordering of society results in the common good (the argument of qualification). For Thomas, persons become virtuous as they promote the common good through a concern for social justice. Similarly, the common good is expressed in the biblical commandment to love God with all of one’s being and to love one’s neighbour as oneself.
In the sixteenth century, Ignatius of Loyola also advocated the common good.[39] The Society of Jesus he founded strove to serve the greater glory of God, which he radically identified with the common good. For Ignatius, the common good was served through the defence and propagation of the Christian faith, but also to education of youths and illiterates, and the compassionate support of prison and hospital inmates. The distinctive contribution of Ignatius to the idea of the common good is his expansion of the vision to embrace all humankind rather than communities or groups with which one might naturally or ideologically identify. Indeed the term “the more universal good” frequently appears in the order’s Constitutions as the criterion by which members of the order should determine what service of God and the church might mean in a given situation.[40]
While the common good was not precisely defined in antiquity, it refers to a normative standard for evaluating the justice of social, legal and political arrangements promoting “the full flourishing of everyone in the community.”[41] The common good may be understood as the common goal of all who promote the justice of a politically organised community, and its achievement, at least in theory, delivers a common sense of fulfilment. A common good may be defined as any good sought and/or enjoyed by two or more persons, but usually a substantial number of persons is in view.[42] A common good may be experienced in isolation but is realised more profoundly when shared in community: “common good includes aggregates of private, individual goods but transcends these aggregates by the unique fulfilment afforded by mutuality, shared activity, and communion of persons.”[43]
Put another way, the common good “describes an environment that is supportive of the development of human potential while safeguarding the community against individual excesses. It looks to the general good, to the good of the many over the interests of the one or the very few.”[44] Or as the Second Vatican Council put it, the common good is “the sum total of social conditions which allow people, either as groups or as individuals, to reach their fulfilment more fully and more easily.”[45] With reference to the discussion of the biblical imperatives outlined above, the Vatican II document further states that “[t]he obligations of justice and love are fulfilled only if each person, contributing to the common good, according to his own abilities and the needs of others, also promotes and assists the public and private institutions dedicated to bettering the conditions of human life.”[46]
The idea of the common good is a leading motif of Catholic social teaching, enshrined in a range of papal, conciliar and other magisterial documents. Australian Catholic theologian Michael Costigan has observed that, “[w]hile, in general, the social teachings are not unique to Roman Catholicism, the Popes and other Church leaders have developed them more systematically than other Churches in the period since 1891, when Pope Leo XIII issued his Encyclical Letter, Rerum Novarum.”[47] In general, Protestant theologians, philosophers and practitioners have accepted the Catholic social teaching as their own, given it a respectful if disinterested nod, or ignored it as inimical to their pragmatic agendas founded on the doctrines of political liberalism and individualism.
The public good is achieved through the aggregation by public institutions of goods characterised by principles such as non-rivalry and non-excludability. Thus, as Hollenbach observes, the enjoyment of a public good by some people does not mean that others cannot enjoy it. Further, if a public good “is there for all, it is there for everyone; if it is present for anyone, it is present for all.”[48] The common good includes, but is not limited to, public goods. According to James B. Murphy, “the common good is best promoted by, in addition to the state, many lower-level non-public societies, associations, and individuals.” This is the application of the principle of subsidiarity. One danger of emphasis on the public good – in contrast to an informed understanding of, and contribution to, the common good – is that neoliberal economists delight in defining public goods in purely economic terms, reframing arguments for social justice to suit the ideological agenda of economic fundamentalists.[49] The common good cannot be reduced to purely economic terms since it includes human relationships of mutuality, affection and non-rivalry – relationships entered into and necessary for their own sake, not merely in order to satisfy some pragmatic end.
Of course, the existence of a very large community, or a plurality of visions for society, might subvert or eclipse the common good.[50] This is the challenge brought by John Rawls in his Political Liberalism.[51] In addition to cultural diversity and pluralism, there are other potential barriers to a successful embrace of the common good in a modern society. For example, there may be disagreement about the extent of commonality, or about what defines “the good.” Moreover, the benefits provided by the common good are distributed indiscriminately, including to those who choose not to contribute to the goal. Another barrier is the extreme individualism championed by many Western nations today, “in which it is difficult, perhaps impossible, to convince people that they should sacrifice some of their freedom, some of their personal goals, and some of their self-interest, for the sake of the common good.”[52] A further barrier is the problem of unequally shared burdens: in order to achieve and maintain the common good, some members of a community will necessarily bear much greater responsibility for the costs than others.
What, then, is the common good? It is analogous to, though not synonymous with, the biblical teaching on justice and shalom, and the Gospel imperative of neighbour-love. It is a principle that seeks to protect a community against the excesses of despotism and individualism. It describes the ideal social conditions for the flourishing and fulfilment of every member of a community. It is the responsibility “to contribute to the development and maintenance of a good and fair society, doing what [one] can for the benefit of everyone – or to say the same thing negatively, doing nothing that will harm anyone.”[53] It enables discussion of the kind of society that is desirable, how such a social reality might be realised, and what contribution one is willing to make to see it take root in the soil of a particular community.
Conclusion
The right to life is a basic human right. The systematic exploitation of poor and oppressed persons for profit/health is a denial of human rights. At what human cost should a person who has access to organ transplantation technology pursue their desire for longevity and wellbeing? At what cost to justice should the state, or medical professionals, allocate organs and tissue? How might more ethical alternatives be defended and employed? Is it possible to speak confidently of universal notions of justice and ethics? The practical issues raised in this paper may be framed in the wider context of biotechnology, bioethics and public theology:[54]
- What priority should the churches give to influencing public policy on bioethical issues, and why?
- What should the churches aim to achieve when they enter public and political debates on these issues?
- What strategies should they employ to achieve their aims?
- What capacity is there among Baptist churches and agencies to employ such strategies and achieve such aims?
A final word: in the 1960s Canadian communications scholar Marshall McLuhan reminded us that we shape our tools, and then they shape us.[55] What was true of communications technology in the twentieth century may well be true of biotechnology in the twenty-first century as it recreates our human world in the image of something both gloriously compelling and subtly contrived.
Technology has the power to destroy what is of value, whether it is physical, political, economic or moral. Technology, and biotechnology in particular, ought to be restrained and constrained by ethical principles established through community consensus and supported in state regulation and legislation, and that have as their goal the common good.
Surely Baptists have much to contribute to such a project.
References
[1] R. Eastern, “A question of consent? The Transplantation and Anatomy Amendment Bill 1998,” Research Bulletin 1/99, pp. 1-2. Parliament of Queensland (Australia).
[2] See, e.g., Tom. L. Beauchamp & James F. Childress, Principles of Biomedical Ethics (fifth edition; Oxford: Oxford University Press, 2001), pp. 57-282.
[3] Australians Donate, “Number of deceased organ donors,” http://www.australiansdonate.org.au/downloads/OrganDonation_InformationKitJuly2005.pdf, p. 2, n.d., found on 13 June 2007.
[4] Newspoll opinion poll, 30 March 2004.
[5] Australians Donate, “Number of deceased organ donors,” p. 3.
[6] Ibid., p. 2.
[7] Andrew Lawrence, “Presumed consent organ donation under Australian law,” paper prepared for the Australian Medical Association and the Australian National University law internship program, June 2004, p. 4.
[8] Australian and New Zealand Organ Donor Registry, 2007 Report, p. 1. http://www.anzdata.org.au/ANZOD/ANZODReport/2007/2007Pages01-20.pdf, found on 13 Jun 2007.
[9] Ibid., p. 3.
[10] Elizabeth King & Russell G. Smith, “Human tissue transplantation crime,” Trends and Issues in Crime and Criminal Justice, Australian Institute of Criminology, May 1998, p. 2.
[11] http://www.medicareaustralia.gov.au/yourhealth/our_services/aodr/how_register.shtml, dated 13 June 2007, found on 13 June 2007.
[12] Five of these issues are noted by James F. Childress, “Organ transplantation,” in John Macquarrie & James F. Childress (eds), Westminster Dictionary of Christian Ethics (Philadelphia: Westminster Press, 1986), pp. 441-443. The issue of foetal tissue is noted in Boronia Halstead & Paul Wilson, ““ ‘Body crime’: Human organ procurement and alternatives to the international black market,” Australian Institute of Criminology Trends & Issues in Crime and Criminal Justice No. 30, Mar 1991, p. 2.
[13] The Sydney Morning Herald, 13 December 1988.
[14] The New York Times, 1 August 1989.
[15] The Guardian, 5 April 1990.
[16] Halstead & Wilson, “‘Body Crime,’” p. 4.
[17] The Sydney Morning Herald, 26 September 1990, citing an article in The Guardian. The article also claimed that “such as trade is also known to exist in Mexico and Thailand.”
[18] Health Issues Centre and Association of District Health Councils of Victoria, Organ Transplants (Melbourne: HIC, 1990), p. 15.
[19] Halstead & Wilson, “‘Body Crime,’” p. 4.
[20] G.M. Abouna et al, “Commercialisation in human organs: A Middle Eastern perspective,” Transplantation Proceedings 22 (3), June 1990, pp. 918-921.
[21] Transplant News (Reuters Australasian Briefing), 31 August 1996.
[22] The Age (Melbourne), 2 March 1998, pp. A1-2.
[23] Association for Asian Research, “Respected surgeon urges others to speak out against forced organ donation in China,” http://www.asianresearch.org/articles/2890.html, dated 25 May 2006, found on 13 May 2007. See also Telegraph (UK), 30 June 2001, http://www.telegraph.co.uk/news/main.jhtml?xml=/news/2001/07/01/wchi01.xml, found on 13 June 2007.
[24] ABC Radio “PM,” 10 July 2006; and http://www.safecom.org.au/news-1107-2006.htm, dated 11 July 2006, found on 13 June 2007.
[25] David Matas & David Kilgour, Bloody Harvest: Revised Report into Allegations of Organ Harvesting of Falun Gong Practitioners in China,
http://organharvestinvestigation.net/report0701/report20070131-eng.pdf, p. 62, dated 31 January 2007, found on 13 June 2007 [note: 7Mb pdf].
[26] See especially “Organ harvesting in China,” dated 20 August 2006, http://www.youtube.com/watch?v=Ia04u0u8J8s; and “Organ selling in China,” dated 2 October 2006, http://www.youtube.com/watch?v=0wtSV_BEf14, found on 13 June 2007.
[27] Neil Messer, Theological Issues in Bioethics: An Introduction with Readings (London: Darton, Longman & Todd, 2002), pp. 191-192.
[28] Ibid., 192.
[29] For example, Isa 28:7; 32:16-17; Hos 2:19-20.
[30] See, for example, Walter Brueggemann, Isaiah 1-39 (Louisville, KY: Westminster John Knox Press, 1998), p. 48; Barbara Johnson, “mishpat,” in G. Johannes Botterweck, H. Ringgren & H.-J. Fabry, Theological Dictionary of the Old Testament (vol. 9; Grand Rapids: Wm B. Eerdmans, 2003), pp. 86-98; and Johnson, “tsedaqah,” in Botterweck et al, op. cit., vol. 12, pp. 239-264.
[31] Donald Guthrie, New Testament Theology (Leicester: IVP, 1981), pp. 945-946.
[32] Duncan B. Forrester, Christian Justice and Public Policy (Cambridge: Cambridge University Press, 1997), p. 208.
[33] John R. Donahue, “The Bible and social justice: ‘Learn to do right! Seek justice’ (Isa 1:17 NIV)”, in Michael J. Gorman (ed.), Scripture: An ecumenical introduction to the Bible and its interpretation (Peabody, MA: Hendrickson Publishers, 2005), p. 240.
[34] M.A. Seifrid, “Righteousness, justice, and justification,” in T.D. Alexander & Brian S. Rosner (eds), New Dictionary of Biblical Theology (Leicester: IVP, 2000), p. 740.
[35] See, for example, Nicholas Wolterstorff, Until Justice and Peace Embrace (Grand Rapids: Wm B. Eerdmans, 1983), especially pp. 69-72.
[36] David Hollenbach, The Common Good and Christian Ethics (Cambridge: Cambridge University Press, 2002), p. 3.
[37] Aristotle, Nichomachean Ethics (trans. Martin Oswald; Indianapolis, IN: Bobbs-Merril, 1962), p. 1049.
[38] Thomas Aquinas, Summa Theologica, 1-2, q. 92 (a) 1, ad 3.
[39] David Hollenbach, Common Good, pp. 5-6.
[40] Ibid.
[41] James Bernard Murphy, “common good,” in Robert Audi (gen. ed.), The Cambridge Dictionary of Philosophy (second edition; Cambridge: Cambridge University Press, 1999), p. 161.
[42] Ibid.
[43] Ibid.
[44] William J. Byron, The Power of Principles: Ethics for the new corporate culture (Maryknoll, NY: Orbis Books, 2006), p. 155.
[45] Walter M. Abbott (ed.), Documents of Vatican II (New York: America Press, 1966), p. 225.
[46] Ibid., p. 228.
[47] Michael Costigan, “Catholic Social Teaching,” a foundation document of the Centre for an Ethical Society, available at http://www.ces.org.au/uploaded/articles/00005.pdf, dated 21 Nov 2006, found on 26 Nov 2006.
[48] Hollenbach, Common Good, p. 8.
[49] Geoff Dornan, “The necessity of and priority for the common good in contemporary Australia: A response to the Leader of the Federal Opposition’s address to the Centre for Independent Studies, November 16th 2006,” Centre for an Ethical Society, http://www.ces.org.au/uploaded/articles/00010.pdf, dated 4 January 2007, found on 17 January 2007.
[50] Hollenbach, Common Good, p. 9.
[51] John Rawls, Political Liberalism (New York: Columbia University Press, 1993). Although, here and elsewhere, Rawls offers important insights into the relations between a commitment to individual liberty and a commitment to communitarianism (and the common good), it is not my intention to critique his argument here.
[52] Manuel Velasquez et al, “The common good,” Issues in Ethics 5 (2), Spring 1992, available at http://www.scu.edu/ethics/practicing/decision/commongood.html, found on 23 May 2007.
[53] Byron, The Power of Principles, p. 152.
[54] Questions 1-3 were posed by the Catholic Bishops of England and Wales in a booklet titled Vote for the Common Good, published in advance of the British General Election in 2001, and reproduced in Messer, Theological Issues in Bioethics, p. 270. The fourth question is one I wish to pose to Baptist leaders.
[55] “The new electronic interdependence recreates the world in the image of a global village,” The Gutenberg Galaxy (Toronto, Canada: University of Toronto Press, 1962), p. 43.
This is a transcript of a paper by Rod Benson, Director of the Centre for Christian Ethics, Morling College, Sydney, Australia, presented to a meeting of the Commission on Christian Ethics, Baptist World Alliance, Accra, Ghana, July 2007.
